
More Information
Submitted: May 27, 2022 | Approved: June 06, 2022 | Published: June 07, 2022
How to cite this article: Karasu M, Karaca O, Kobat MA, Kıvrak T, İpek MI. The effect of frequency of sexual intercourse on coronary artery disease. Arch Vas Med. 2022; 6: 001-004.
DOI: 10.29328/journal.avm.1001015
Copyright License: © 2022 Karasu M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Coronary artery disease; Sexual intercourse

The effect of frequency of sexual intercourse on coronary artery disease
Mehdi Karasu1* , Özkan Karaca1, Mehmet Ali Kobat1, Tarık Kıvrak1 and Mehmet İkbal İpek2
, Özkan Karaca1, Mehmet Ali Kobat1, Tarık Kıvrak1 and Mehmet İkbal İpek2
1Department of Cardiology, Firat University Hospital, Turkey
2Department of Urology, Firat University Hospital, Turkey
*Address for Correspondence: Mehdi Karasu, Department of Cardiology, Firat University Hospital, Turkey, Email: [email protected]
Background: Doubts about the safety of sexual activity are common among cardiac patients and physicians alike, and are often neglected during routine checkups or on discharge from the hospital following a cardiac event or invasive procedure. Although it varies from society to society, it is considered taboo by most patients, so it is reluctant to ask the doctor about sexual activity. Doctors, on the other hand, remain silent due to the lack of clear information about the effect of sexual activity on coronary artery diseases or the presence of doubts. It is ultimately set aside by professionals and their patients. The patient does not ask and the doctor does not answer. This study, it was aimed to investigate the effect of the frequency of sexual intercourse on coronary artery disease.
Methods: After applying the exclusion criteria, the remaining 180 patients were included in the study. A self-administered survey was applied to the patients before coronary angiography and patients were assessed according to the presence of additional diseases, their demographic characteristics, and the frequency of sexual intercourse. Two experienced physicians evaluated the angiographic results. Firstly Patients were grouped as 90 patients with normal coronary anatomy and 90 patients with coronary artery disease. After this, Coronary artery disease severity was evaluated according to syntax score.
Results: The mean age of the patients was 58 ± 12.5 years. The distribution of age is not reasonable. According to gender, the female/male ratio the proportion of men was higher in patients with coronary artery disease. İncidence of normal coronary anatomy increased as the frequency of sexual intercourse increased. P - value was 0.037 and the result was statistically significant. The frequency of sexual intercourse was found to be 4.2/per month. The relationship between the Syntax score and frequency of sexual intercourse was not statistically significant (p > 0.05).
Conclusion: As a result of the study, it was seen that patients with more frequent sexual intercourse had more normal coronary artery anatomy, and those with coronary artery disease had single coronary artery disease than multiple vascular disorders. it was concluded that the incidence of coronary artery disease and coronary artery disease severity decreased as the frequency of sexual intercourse increased. Sexual intercourse might be a preventive factor in the development of coronary artery disease.
Coronary artery disease is one of the most common causes of death in the world [1]. The leading cause of coronary artery disease is atherosclerosis. It emerges and progresses as a result of a progressive process under the influence of environmental and genetic factors [2].
As an outstanding example, the frequency of sexual intercourse can be evaluated as one of the health indicators, and sexual dysfunction has many common mechanisms with coronary artery disease pathology [3]. The atherosclerotic process may not only occur in one region of the arterial network but may commonly involve many tissues and organs. For example, a person with coronary artery disease may develop the cerebrovascular disease, peripheral artery disease, pulmonary arterial disease, and erectile dysfunction at the same time or in the course of time. Various studies have shown a relationship between erectile dysfunction and coronary artery disease [4-6].
Patients followed up with acute coronary syndrome may have a low sexual function, sometimes due to the side effects of the drugs used, sometimes due to the anxiety and fear of the present disease on partners, and sometimes because of the inadequate and suspicious approach of doctors on this subject [7].
Although estrogen is predominantly in the premenopausal period, in other words, when they have the adequate sexual functional capacity, it is known that in this period, coronary artery disease is rarer in women than in the postmenopausal period [8]. However, there was no positive effect of hormone replacement therapy on coronary artery disease. Some studies on testosterone, some studies have shown that testosterone replacement therapy harms coronary artery disease [9]. However, in some studies, it was observed that erectile dysfunction, loss of libido, and a decrease in the frequency of sexual intercourse increase the 10-year cardiovascular risk in hypogonadal men [10].
In general, it is recommended that patients who have cardiovascular risk factors or who apply for health care with acute coronary syndrome should be avoided heavy exercise and avoid intense sexual intercourse. The aim of our study is to investigate the possible psychosomatic effects of sexual intercourse on coronary artery disease and to help people with coronary artery disease in terms of sexual counseling according to the results.
Our study was conducted as a thesis study on patients who were admitted to the outpatient clinic of Fırat University Medical Faculty Hospital between March 2018 and June 2018 and decided to have coronary angiography. Before the study, the approval of the Ethics Committee for Scientific Research of Fırat University Faculty of Medicine was obtained. Two experienced physicians evaluated the angiographic results of the patients. Coronary artery disease severity was evaluated according to the syntax score. Patients were assessed according to risk factors and general demographic characteristics of coronary artery disease. The patients were asked about age, sex, DM, HT, smoking, alcohol, SVH (Cerebro Vascular Disease), CRF (Chronic Renal Failure), and IHD (Ischemic Heart Disease) in the family, occupation, educational status, and a number of satisfactory sexual intercourse per month.
Exclusion criteria were as follows
Patients who have erectile dysfunction (The International Scale of Erectile Function (IIEF) was used to evaluate erectile dysfunction. Female sexual dysfunction was evaluated according to the Female Sexual Function Index), patients who did not have sexual partners, patients who had undergone coronary stenting, patients who did not want to answer the question of the frequency of sexual intercourse for privacy, patients using PDE5I and B blocker-like drugs that affect the sexual activity and patients with systemic disease previously shown to affect erectile dysfunction, such as DM were excluded from the study. The patients were evaluated regardless of gender differences and they were asked to say the number of satisfactory sexual intercourse. Evaluating of sexual intercourse questions was done by a urologist who was not aware of the angio information of the patients.
Statistical analysis
Data were analyzed with Windows SPSS software version 22.0. Descriptive statistics were used for values such as frequency, mean, standard deviation, median, and range. The Chi-Square test was used to compare the qualitative variables between the independent groups of more than three groups, and the expected values were less than 5 in the evaluation of the study groups according to different variables. The sample T-test was used to determine the significance of the difference between two means in two independent groups. To be statistically significant, the p - value was accepted as less than 0.05 for all data.
The mean age of the patients was 58 ± 12.5 years. The distribution of age is not reasonable (Table 1). The clinical and demographic characteristics of the patients are given in Table 2. The p - value of the relationship between age and coronary artery disease was statistically significant (Figure 1). The proportion of men was higher in patients with coronary artery disease. Non-critical coronary artery stenosis, single-vessel disease, and multivessel disease were the most commonly seen in housewives in retired people. The frequency of sexual intercourse was found to be 4.2/month (Table 3).
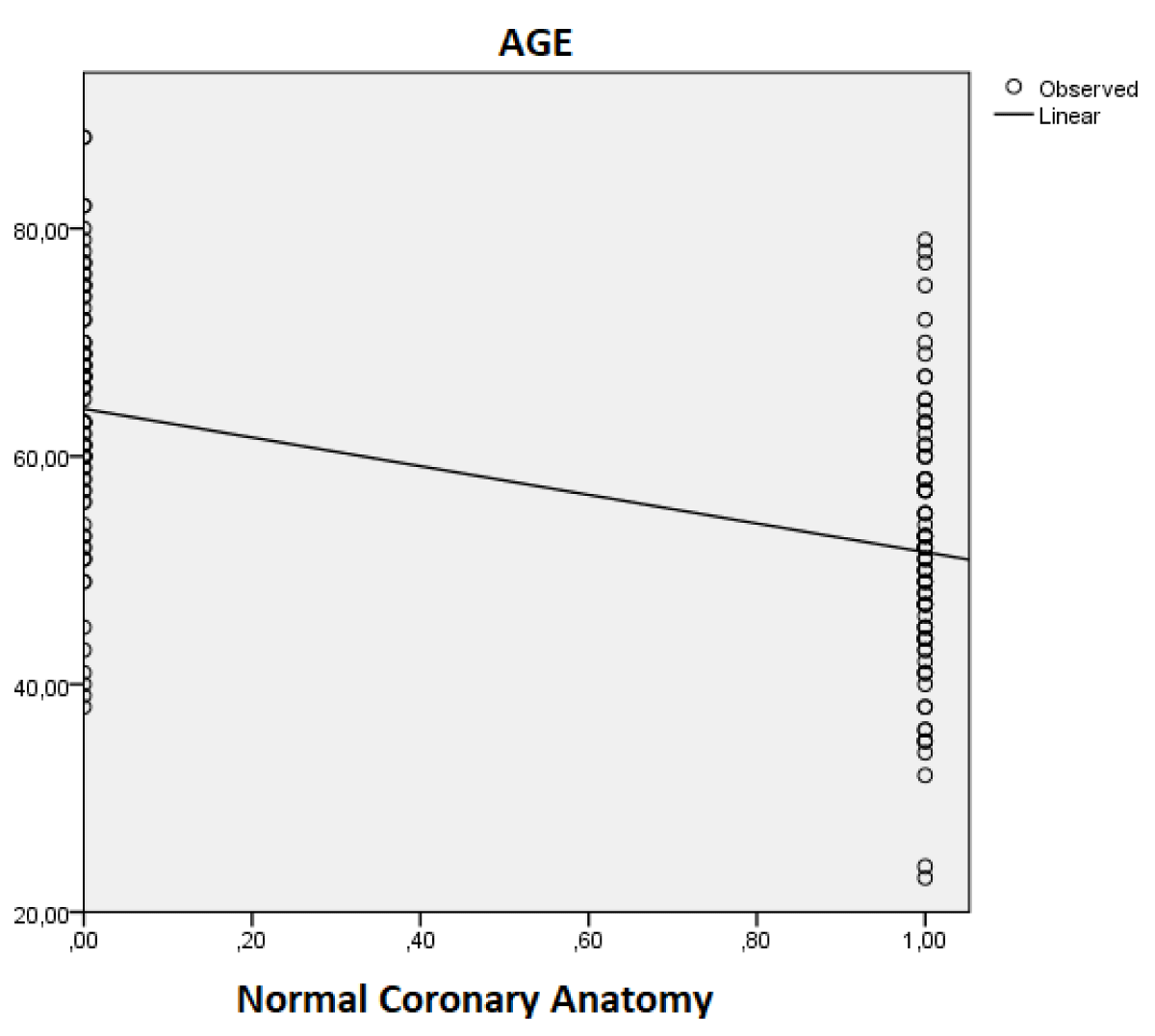
Figure 1: Distribution of age according to the presence of coronary artery disease.
| Table 1: Demographic and clinical characteristics of the general population. | |||
| Demographic and clinical characteristics | n | % | Current percentage |
| DM | 48 | 26.7 | 26.7 |
| HT | 80 | 44.4 | 44.4 |
| Cigarette | 48 | 26.7 | 26.7 |
| Alcohol | 5 | 2.8 | 2.8 |
| CVD | 4 | 2.2 | 2.2 |
| CRF | 14 | 7.8 | 7.8 |
| IHD in family | 56 | 31.1 | 31.1 |
| Table 2: Comparison of demographic and clinical characteristics according to the presence of coronary artery disease. | |||
| Demographic and clinical characteristics | NCA | Coronary Artery Disease | p value |
| Age | 51.9 ± 11 | 64.1 ± 10 | 0. 000 |
| Gender (F/M) | 50/40 (%27.7/22.2) | 29 (%16.1) / 61 (%33.8) | 0. 001 |
| HT | 27 (%15) | 53 (%29.9) | 0. 000 |
| DM | 13 (%7.2) | 35 (%19.4) | 0. 000 |
| Cigarette | 20 (%11.1) | 28 (%15.5) | 0. 231 |
| IHD in family | 6 (%3.3) | 49 (%27.2) | 0. 000 |
| Alcohol | 4 (%2.2) | 1 (%0.5) | 0. 176 |
| CRF | 2 (%1.1) | 12 (%6.6) | 0. 005 |
| CVD | 0 (%0) | 4 (%2.2) | 0. 043 |
| Table 3: Frequency of sexual intercourse. | ||
| Number | Current | 180 |
| Mean Value | 4. 2056 | |
In the comparison of the relationship between the rate of sexual intercourse and the severity of coronary artery disease, the mean value of sexual intercourse was 4.2/month, and the upper integer value of 5 was taken as the threshold (Table 4).
| Table 4: Distribution of the frequency of sexual intercourse 5 and above and below 5 according to the severity of coronary artery disease. | ||
| Frequency of sexual intercourse | N | |
| NCA | > = 5. 00 | 38 |
| < 5. 00 | 52 | |
| Noncritical | > = 5. 00 | 8 |
| < 5. 00 | 26 | |
| Single-vessel | >= 5. 00 | 7 |
| < 5. 00 | 28 | |
| Multiple vessel | >= 5. 00 | 3 |
| < 5. 00 | 19 | |
İncidence of normal coronary anatomy increased as the frequency of sexual intercourse increased (Figure 2). P - value was 0.037 and the result was statistically significant (Table 5).
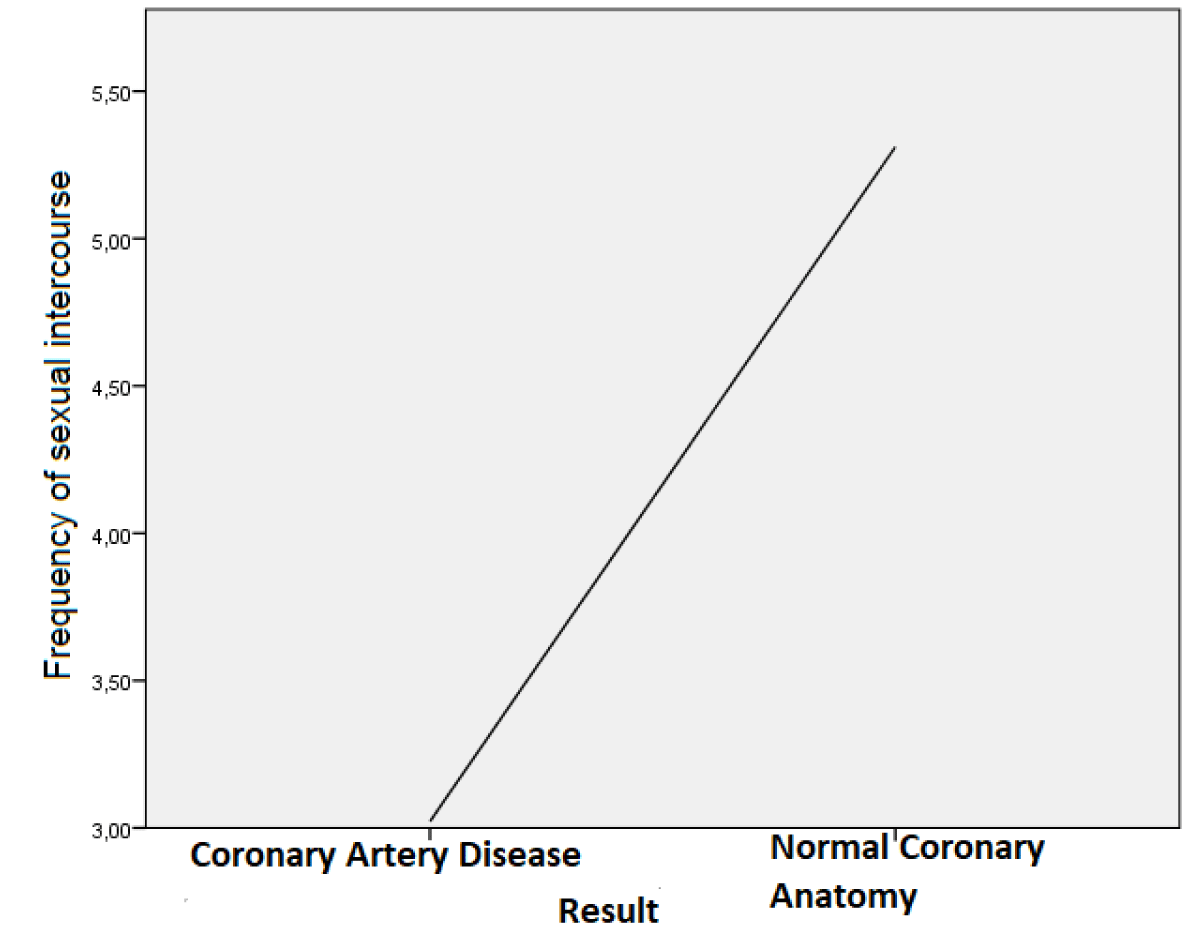
Figure 2: Frequency of sexual intercourse according to coronary artery disease and normal coronary anatomy.
| Table 5: Comparison of frequency of sexual intercourse and coronary artery disease group and normal coronary anatomy group. | |||||
| Result | Total | ||||
| Coronary artery disease | Normal Coronary Anatomi | ||||
| Frequency of Sexual Intercourse | 0 | Number | 31 | 19 | 50 |
| The frequency of sexual intercourse % | 62.0% | 38. 0% | 100.0% | ||
| 1 | Number | 8 | 5 | 13 | |
| The frequency of sexual intercourse % | 61.5% | 38. 5% | 100.0% | ||
| 2 | Number | 16 | 5 | 21 | |
| The frequency of sexual intercourse % | 76.2% | 23. 8% | 100.0% | ||
| 3 | Number | 5 | 7 | 12 | |
| The frequency of sexual intercourse % | 41.7% | 58. 3% | 100.0% | ||
| 4 | Number | 12 | 17 | 29 | |
| The frequency of sexual intercourse % | 41.4% | 58.6% | 100.0% | ||
| 5 | Number | 3 | 2 | 5 | |
| The frequency of sexual intercourse % | 60.0% | 40. 0% | 100.0% | ||
| 6 | Number | 1 | 2 | 3 | |
| The frequency of sexual intercourse % | 33.3% | 66.7% | 100.0% | ||
| 7 | Number | 0 | 2 | 2 | |
| The frequency of sexual intercourse % | 0.0% | 100.0% | 100.0% | ||
| 8 | Number | 6 | 9 | 15 | |
| The frequency of sexual intercourse % | 40.0% | 60.0% | 100. 0% | ||
| 10 | Number | 2 | 5 | 7 | |
| The frequency of sexual intercourse % | 28.6% | 71.4% | 100.0% | ||
| 12 | Number | 4 | 14 | 18 | |
| The frequency of sexual intercourse % | 22.2% | 77.8% | 100.0% | ||
| 16 | Number | 2 | 3 | 5 | |
| The frequency of sexual intercourse % | 40.0% | 60.0% | 100.0% | ||
| Total | Number | 90 | 90 | 180 | |
| The frequency of sexual intercourse % | 50.0% | 50.0% | 100.0% | ||
In the syntax scores calculated by monitoring coronary angiography images of 57 patients with single-vessel and multivessel disease, the highest value was 48, and the lowest cost was 0. The mean value was calculated as 12.3 (Table 6).
| Table 6: Syntax score distribution parameters. | ||||||
| N | Min | Max | Sum | X | SS | |
| Syntax Score | 57 | .00 | 48.00 | 705.50 | 12. 3772 | 9. 43411 |
In our study, it was found that the relationship between coronary artery disease and classic risk factors with coronary artery disease increased with age, and the relationship between sexual activity and coronary artery disease was similar to the results in the literature [11-13]. In our study, gender restriction was not made in the population to take into account not only erectile dysfunction in men but also sexual dysfunction in women. İt was seen that coronary artery disease decreased with a higher frequency of sexual intercourse. The effect of classical risk factors on coronary artery disease was found to be similar to the literature studies. Also, a significant correlation was not found between the syntax score and the frequency of sexual intercourse it was thought that the small number of patients participating in the study was effective in this.
As a result of our research, it was found that the incidence of coronary artery disease decreased with the increasing frequency of sexual intercourse or that coronary artery disease was less severe in individuals with a higher rate of sexual intercourse.
The single-centered study and the relatively small number of patients were the most critical limitations of the study. To make these data more reliable and acceptable, multicentre studies with a higher number of patients are needed. Another limitation of our study is that we did not have an international questionnaire for sexual intercourse.
Although our study supports the conclusion that sexual intercourse may be a preventive factor in the development of coronary artery disease, prospective controlled studies with longer series are needed.
- World Health Organization. Making a difference. Geneva. 1999.
- Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999 Jan 14;340(2):115-26. doi: 10.1056/NEJM199901143400207. PMID: 9887164.
- Imprialos KP, Stavropoulos K, Doumas M, Tziomalos K, Karagiannis A, Athyros VG. Sexual Dysfunction, Cardiovascular Risk and Effects of Pharmacotherapy. Curr Vasc Pharmacol. 2018 Jan 26;16(2):130-142. doi: 10.2174/1570161115666170609101502. PMID: 28595561.
- Montorsi F, Briganti A, Salonia A, Rigatti P, Margonato A, Macchi A, Galli S, Ravagnani PM, Montorsi P. Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery disease. Eur Urol. 2003 Sep;44(3):360-4; discussion 364-5. doi: 10.1016/s0302-2838(03)00305-1. PMID: 12932937.
- Dostálová G, Hlubocká Z, Bayerová K, Bělohlávek J, Linhart A, Karetová D. Erectile Dysfunction in Young Myocardial Infarction Survivors: Evaluation, Follow Up. Am J Mens Health. 2017 Nov;11(6):1739-1744. doi: 10.1177/1557988317714359. Epub 2017 Jul 11. PMID: 28697641; PMCID: PMC5675271.
- Sangiorgi G, Pizzuto A, Diehm N, Greco F, Fusco F, Chiricolo G, Vismara A, Altieri VM, Cereda A, Bongo S. Endovascular therapy for erectile dysfunction: current knowledge and future perspectives. Minerva Cardiol Angiol. 2021 Oct;69(5):579-595. doi: 10.23736/S2724-5683.20.05136-1. Epub 2020 Jun 2. PMID: 32492987.
- Salehian R, Khodaeifar F, Naserbakht M, Meybodi A. Attitudes and Performance of Cardiologists Toward Sexual Issues in Cardiovascular Patients. Sex Med. 2017 Mar;5(1):e44-e53. doi: 10.1016/j.esxm.2016.09.002. Epub 2016 Dec 14. PMID: 27988217; PMCID: PMC5302380.
- Zhu X, Bonet B, Gillenwater H, Knopp RH. Opposing effects of estrogen and progestins on LDL oxidation and vascular wall cytotoxicity: implications for atherogenesis. Proc Soc Exp Biol Med. 1999 Dec;222(3):214-21. doi: 10.1046/j.1525-1373.1999.d01-138.x. PMID: 10601880.
- Elsherbiny A, Tricomi M, Bhatt D, Dandapantula HK. State-of-the-Art: a Review of Cardiovascular Effects of Testosterone Replacement Therapy in Adult Males. Curr Cardiol Rep. 2017 Apr;19(4):35. doi: 10.1007/s11886-017-0838-x. PMID: 28361372.
- Ho CH, Wu CC, Chen KC, Jaw FS, Yu HJ, Liu SP. Erectile dysfunction, loss of libido and low sexual frequency increase the risk of cardiovascular disease in men with low testosterone. Aging Male. 2016 Jun;19(2):96-101. doi: 10.3109/13685538.2015.1129400. Epub 2016 Jan 11. PMID: 26755067.
- Kumar J, Bhatia T, Kapoor A, Ranjan P, Srivastava A, Sinha A, Kumar S, Garg N, Tewari S, Kapoor R, Goel PK. Erectile dysfunction precedes and is associated with severity of coronary artery disease among Asian Indians. J Sex Med. 2013 May;10(5):1372-9. doi: 10.1111/jsm.12041. Epub 2013 Jan 24. PMID: 23347017.
- Feldman DI, Cainzos-Achirica M, Billups KL, DeFilippis AP, Chitaley K, Greenland P, Stein JH, Budoff MJ, Dardari Z, Miner M, Blumenthal RS, Nasir K, Blaha MJ. Subclinical Vascular Disease and Subsequent Erectile Dysfunction: The Multiethnic Study of Atherosclerosis (MESA). Clin Cardiol. 2016 May;39(5):291-8. doi: 10.1002/clc.22530. Epub 2016 May 3. PMID: 27145089; PMCID: PMC4879072.
- Hodges LD, Kirby M, Solanki J, O'Donnell J, Brodie DA. The temporal relationship between erectile dysfunction and cardiovascular disease. Int J Clin Pract. 2007 Dec;61(12):2019-25. doi: 10.1111/j.1742-1241.2007.01629.x. PMID: 17997808.